Potrebbero piacerti anche
- Guide to Canine and Feline ElectrocardiographyDa EverandGuide to Canine and Feline ElectrocardiographyRuth WillisNessuna valutazione finora
- PacemakerDocumento39 paginePacemakerb7bkroroNessuna valutazione finora
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Da EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Nessuna valutazione finora
- PacemakerDocumento52 paginePacemakerPraveena RNessuna valutazione finora
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocumento50 pagineCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNessuna valutazione finora
- Mechanisme ArrhythmiaDocumento38 pagineMechanisme ArrhythmiarskdemergencyNessuna valutazione finora
- PacemakerDocumento63 paginePacemakerMonish RautNessuna valutazione finora
- ECG Basics: Understanding Waves, Intervals and LeadsDocumento12 pagineECG Basics: Understanding Waves, Intervals and LeadsAprina RosyadahNessuna valutazione finora
- Electro Cardiograph yDocumento94 pagineElectro Cardiograph ykajonasfoodproductsNessuna valutazione finora
- Tomasz WikarekDocumento95 pagineTomasz Wikareknamar13766Nessuna valutazione finora
- PacemakerDocumento156 paginePacemakerDhruv DesaiNessuna valutazione finora
- N12 Cardiac DysrhythmiasDocumento68 pagineN12 Cardiac Dysrhythmiaskathbondoc03Nessuna valutazione finora
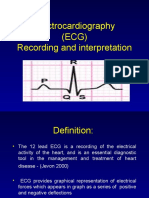
- Electrocardiography (ECG) Recording and InterpretationDocumento59 pagineElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- PacemakersDocumento45 paginePacemakersFatos SylajNessuna valutazione finora
- Basic of ECG: Prepared By: Zahid HussainDocumento38 pagineBasic of ECG: Prepared By: Zahid HussainZahid Hussain100% (1)
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocumento74 pagineBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- Temporary Cardiac Pacing GuideDocumento49 pagineTemporary Cardiac Pacing GuidevaishnaviNessuna valutazione finora
- Ecg in ExDocumento70 pagineEcg in ExLakshmi PrasannaNessuna valutazione finora
- Electrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHDocumento42 pagineElectrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHNorPhea - នភាNessuna valutazione finora
- Romeo Mathew: Clinical Instructor MconDocumento36 pagineRomeo Mathew: Clinical Instructor MconRomeo MathewNessuna valutazione finora
- Dr. Anas Yasin - MDDocumento58 pagineDr. Anas Yasin - MDMahfouzNessuna valutazione finora
- ECGs The Basics (Part 1) LectureDocumento32 pagineECGs The Basics (Part 1) Lectureliudmyla zakordonetsNessuna valutazione finora
- Ecgs Full For Ad2 2023 Ek Am KGDocumento29 pagineEcgs Full For Ad2 2023 Ek Am KGj7g2m8fjqvNessuna valutazione finora
- Hemodynamic MonitoringDocumento34 pagineHemodynamic Monitoringkurt94764Nessuna valutazione finora
- ECGs The Basics (Part 1) LectureDocumento33 pagineECGs The Basics (Part 1) Lectureliudmyla zakordonetsNessuna valutazione finora
- ECG Complete LectureDocumento33 pagineECG Complete LectureDr. SUVA NATHNessuna valutazione finora
- EKG 12 Lead GuideDocumento59 pagineEKG 12 Lead GuideM Lukman HakimNessuna valutazione finora
- ECG UpdatedDocumento115 pagineECG Updatedmominarasool7Nessuna valutazione finora
- Chapter - 036 Arrhythmias ClassDocumento129 pagineChapter - 036 Arrhythmias ClassWisdomIsMiseryNessuna valutazione finora
- Asist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasDocumento64 pagineAsist. Univ. Dr. Mihaela Popescu Catedra de Cardiologie Spitalul Universitar de Urgenta EliasAnonymous CQmrhq1O7Nessuna valutazione finora
- MUCLecture 2021 1292271Documento34 pagineMUCLecture 2021 1292271Kouka MahfoudiNessuna valutazione finora
- Cardiac Pacemaker: BY E.DeepikaDocumento17 pagineCardiac Pacemaker: BY E.Deepikadeepika_164Nessuna valutazione finora
- NURV 456 Telemetry Interpretation StudentDocumento56 pagineNURV 456 Telemetry Interpretation StudentMarie Yi100% (2)
- Basics of EKG InterpretationDocumento132 pagineBasics of EKG InterpretationArif Imam HidayatNessuna valutazione finora
- Ecg Interpretation: Gowtham Krishna JDocumento60 pagineEcg Interpretation: Gowtham Krishna JGowtham KrishnaNessuna valutazione finora
- Ecg Treadmill and Holter TestDocumento77 pagineEcg Treadmill and Holter TestRiteka Singh100% (1)
- For Final YearDocumento40 pagineFor Final YearSalman KhanNessuna valutazione finora
- Cardiocon ECG Workshop Basics of ECGDocumento80 pagineCardiocon ECG Workshop Basics of ECGshazia kaziNessuna valutazione finora
- Cathlab Hemodynamics - Pressures, Waveforms, Cardiac Output and ResistanceDocumento33 pagineCathlab Hemodynamics - Pressures, Waveforms, Cardiac Output and Resistancesubha shreeNessuna valutazione finora
- Basic ECG LectureDocumento148 pagineBasic ECG LectureAradhanaRamchandaniNessuna valutazione finora
- ECG-EKG Presentation - Gunda GDocumento21 pagineECG-EKG Presentation - Gunda GGadzikaNessuna valutazione finora
- APEC 611 Scientific and Industrial Instrumentation: Electrocardiogram (ECG)Documento22 pagineAPEC 611 Scientific and Industrial Instrumentation: Electrocardiogram (ECG)Faisal Bin KashemNessuna valutazione finora
- PacemakerDocumento24 paginePacemakerLAWKUSH KUMARNessuna valutazione finora
- Normal Sinus RhythmDocumento48 pagineNormal Sinus RhythmStella mNessuna valutazione finora
- Aritmia LetalDocumento49 pagineAritmia LetalfebriyakNessuna valutazione finora
- Dr Andika Sitepu Departemen Kardiologi dan Vaskuler FKUI National Cardiac Center Harapan Kita Jakarta EKGDocumento45 pagineDr Andika Sitepu Departemen Kardiologi dan Vaskuler FKUI National Cardiac Center Harapan Kita Jakarta EKGJenny CandraNessuna valutazione finora
- ECG Guide: Everything You Need to Know About ElectrocardiogramsDocumento72 pagineECG Guide: Everything You Need to Know About ElectrocardiogramsGaras AnnaBerniceNessuna valutazione finora
- Kuliah EKG Blok Kegawatdaruratan September 2018Documento122 pagineKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNessuna valutazione finora
- PacemakersDocumento69 paginePacemakersdocjeevan89100% (1)
- Basics of EKG InterpretationDocumento132 pagineBasics of EKG InterpretationSiddhant GautamNessuna valutazione finora
- ELECTROCARDIOGRAMDocumento63 pagineELECTROCARDIOGRAMMbah GapinbissiNessuna valutazione finora
- ECG InterpretationDocumento73 pagineECG Interpretationsultan khabeebNessuna valutazione finora
- Cardiovascular Physiology:: Circuitry, Hemodynamics, ElectrophysiologyDocumento27 pagineCardiovascular Physiology:: Circuitry, Hemodynamics, Electrophysiologyrsmoney3Nessuna valutazione finora
- Basic EKG InterpretationDocumento48 pagineBasic EKG InterpretationAimee Ann Pauco MacaraegNessuna valutazione finora
- Ecg Crit - CareDocumento55 pagineEcg Crit - CarekrismatactayNessuna valutazione finora
- Pacemaker: by Azaz KhanDocumento76 paginePacemaker: by Azaz KhanRitaLakhaniNessuna valutazione finora
- Module - 1 EkgDocumento11 pagineModule - 1 EkgCarmen CiursaşNessuna valutazione finora
- THE NORMAL ELECTROCARDIOGRAM: DIAGNOSING MEDICAL PROBLEMS WITH AN ECGDocumento63 pagineTHE NORMAL ELECTROCARDIOGRAM: DIAGNOSING MEDICAL PROBLEMS WITH AN ECGPuravin Crishan VeerasamyNessuna valutazione finora
- Permanent Pacemaker: Supervisor: DR Pipin Ardhianto SPJP (K), FihaDocumento67 paginePermanent Pacemaker: Supervisor: DR Pipin Ardhianto SPJP (K), Fihapelantikan ppnirsdkNessuna valutazione finora
- Core V - Cardiovascular CoreDocumento35 pagineCore V - Cardiovascular CoreMatthew LeiNessuna valutazione finora
- Circulatory System WoowowowoDocumento31 pagineCirculatory System Woowowowosnoops moopsNessuna valutazione finora
- 2019 - SAGE - MICS Aortic Valve Replacement With Sutureless Valves, International Prospective RegistryDocumento11 pagine2019 - SAGE - MICS Aortic Valve Replacement With Sutureless Valves, International Prospective RegistryOmán P. Jiménez A.Nessuna valutazione finora
- Left-Sided Heart FailureDocumento3 pagineLeft-Sided Heart FailureKhalid Mahmud ArifinNessuna valutazione finora
- A Practical Guide To Hemiplegia TreatmentDocumento528 pagineA Practical Guide To Hemiplegia TreatmentSpineCare Physiotherapy100% (2)
- Ecg Made Ridiculously Easy!Documento78 pagineEcg Made Ridiculously Easy!momobelle100% (8)
- Anatomy and Physiology: Placement: First YearDocumento12 pagineAnatomy and Physiology: Placement: First YearJerin CyriacNessuna valutazione finora
- Management of Patients With Structural Infections and Inflammatory Cardiac Disorders Hinkle PPT CH 28Documento50 pagineManagement of Patients With Structural Infections and Inflammatory Cardiac Disorders Hinkle PPT CH 28DelindaEvans100% (4)
- How The Lungs Work?Documento1 paginaHow The Lungs Work?John Marlo CatibogNessuna valutazione finora
- Shunt Calculation, NICVDDocumento31 pagineShunt Calculation, NICVDNavojit ChowdhuryNessuna valutazione finora
- Cardiovascular EmergenciesDocumento2 pagineCardiovascular EmergenciesAli AbdullahiNessuna valutazione finora
- Mastering Electocardiograms - Honda-2Documento3 pagineMastering Electocardiograms - Honda-2Christian MacielNessuna valutazione finora
- Congenitally Corrected Transposition of The Great Arteries (CcTGA)Documento9 pagineCongenitally Corrected Transposition of The Great Arteries (CcTGA)andinarangNessuna valutazione finora
- ANP 1105 The Lymphatic SystemDocumento23 pagineANP 1105 The Lymphatic SystemMathios TigerosNessuna valutazione finora
- Echo Guidelines For Chamber QuantificationDocumento24 pagineEcho Guidelines For Chamber QuantificationOnon EssayedNessuna valutazione finora
- Anatomy and Physiology of Farm AnimalsDocumento157 pagineAnatomy and Physiology of Farm AnimalsOliver Talip100% (1)
- 6 - Skill 3Documento4 pagine6 - Skill 3Adistya VirginNessuna valutazione finora
- Percutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookDocumento18 paginePercutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookRanda TabbahNessuna valutazione finora
- CPAIM Couse SyllabusDocumento48 pagineCPAIM Couse SyllabussajidtoshibaNessuna valutazione finora
- A Drug Study On Evening Primrose OilDocumento5 pagineA Drug Study On Evening Primrose OilthisiskhalylNessuna valutazione finora
- Unit I (Hypertension) Part 1Documento77 pagineUnit I (Hypertension) Part 1RUSSEL JAN ROJASNessuna valutazione finora
- Coronary Angiography: A Continuing Education ProgramDocumento71 pagineCoronary Angiography: A Continuing Education ProgramVincha R LuqmanNessuna valutazione finora
- Cardiovascular System: Related Kidshealth LinksDocumento6 pagineCardiovascular System: Related Kidshealth LinkslaupowerNessuna valutazione finora
- Structure of Blood Vessels - StationsDocumento6 pagineStructure of Blood Vessels - StationsRamya MalariniNessuna valutazione finora
- Veterinary AnatomyDocumento4 pagineVeterinary AnatomyDrRakesh Raki50% (2)
- Cardiac CatheterizationDocumento6 pagineCardiac CatheterizationUzma KhanNessuna valutazione finora
- Trehan 2003Documento5 pagineTrehan 2003Adhitia BudyNessuna valutazione finora
- Syllabi for Civil Services ExamsDocumento128 pagineSyllabi for Civil Services ExamskanhaiyaNessuna valutazione finora
- Pediatric Cardiology PDFDocumento382 paginePediatric Cardiology PDFfarzadfusion100% (5)
- Name - Period - AP Biology Date - Raven Chapter 44 Guided Notes: Circulation & Respiration CirculationDocumento8 pagineName - Period - AP Biology Date - Raven Chapter 44 Guided Notes: Circulation & Respiration CirculationDBQNessuna valutazione finora
- Biology Quiz 1 ReviewDocumento5 pagineBiology Quiz 1 ReviewEllie PamintuanNessuna valutazione finora