Potrebbero piacerti anche
- CAMERON Current Surgical Therapy, Thirteenth EditionDocumento1.667 pagineCAMERON Current Surgical Therapy, Thirteenth Editionniberev100% (2)
- BoneDocumento68 pagineBonedr_asaleh100% (2)
- Response To Civil ClaimDocumento9 pagineResponse To Civil ClaimCanadian Society for the Advancement of Science in Public Policy0% (1)
- Urinary Incontinence in WomenDocumento6 pagineUrinary Incontinence in WomenManju GalagangodageNessuna valutazione finora
- Urogynecology Examination: Divisi Uroginekologi Rekonstruksi Departemen Obstetri Dan Ginekologi Fkui/ RSCMDocumento19 pagineUrogynecology Examination: Divisi Uroginekologi Rekonstruksi Departemen Obstetri Dan Ginekologi Fkui/ RSCMjuanda raynaldi100% (1)
- Contraception: Operational Obstetrics & Gynecology Bureau of Medicine and Surgery 2000 Slide 1Documento14 pagineContraception: Operational Obstetrics & Gynecology Bureau of Medicine and Surgery 2000 Slide 1Robby Prama YudhaNessuna valutazione finora
- NeckDocumento67 pagineNeckdr_asaleh100% (1)
- Paediatric OrthopaedicDocumento77 paginePaediatric Orthopaedicdr_asalehNessuna valutazione finora
- Benign Prostatic HypertrophyDocumento111 pagineBenign Prostatic HypertrophyOnkar SinghNessuna valutazione finora
- Contraceptive ImplantsDocumento17 pagineContraceptive ImplantsKingBee1123Nessuna valutazione finora
- Menstrual Disorder and Abnormal BleedingDocumento9 pagineMenstrual Disorder and Abnormal Bleedingdr_asalehNessuna valutazione finora
- Menstrual Cycle: Prepared By: Mrs Bini P S Amuel Assistant Professor, SSRC N, VapiDocumento16 pagineMenstrual Cycle: Prepared By: Mrs Bini P S Amuel Assistant Professor, SSRC N, VapiBini Don DanielNessuna valutazione finora
- Chronic Pelvic Pain2010Documento48 pagineChronic Pelvic Pain2010Feruza SultanmuratovaNessuna valutazione finora
- Breast LumpDocumento26 pagineBreast Lumpdr_asaleh100% (2)
- Infertility IDocumento36 pagineInfertility Idr_asaleh100% (1)
- Infertility IDocumento36 pagineInfertility Idr_asaleh100% (1)
- Urinary IncontinenceDocumento16 pagineUrinary IncontinenceOana BalintNessuna valutazione finora
- Emergencies in UrologyDocumento112 pagineEmergencies in UrologyafiwahyuNessuna valutazione finora
- TendinitisDocumento7 pagineTendinitisIceLeg SamUelNessuna valutazione finora
- Bladder Injury PDFDocumento7 pagineBladder Injury PDFaaaNessuna valutazione finora
- Novel Coronavirus Disease (COVID-19) Part I: Emergency Department (ED)Documento8 pagineNovel Coronavirus Disease (COVID-19) Part I: Emergency Department (ED)Uzumaki K100% (1)
- Instrumental Vaginal Delivery: Professor Roshan Ara QaziDocumento27 pagineInstrumental Vaginal Delivery: Professor Roshan Ara Qazikaram008Nessuna valutazione finora
- 39-Assessment of Fetal Well BeingDocumento34 pagine39-Assessment of Fetal Well Beingdr_asalehNessuna valutazione finora
- Pujo / UpjoDocumento39 paginePujo / UpjoHafizur RashidNessuna valutazione finora
- Laparascopic Uterine ElevatorDocumento4 pagineLaparascopic Uterine Elevatorgeorgeloto12Nessuna valutazione finora
- Maternal and Child Heath: Jay Pee C. Malibiran Nurse 1 RNDocumento36 pagineMaternal and Child Heath: Jay Pee C. Malibiran Nurse 1 RNRosebel Lagura100% (1)
- (New Paradigms in Healthcare) Maria Giulia Marini, Jonathan McFarland - Health Humanities For Quality of Care in Times of COVID - 19-Springer (2022)Documento175 pagine(New Paradigms in Healthcare) Maria Giulia Marini, Jonathan McFarland - Health Humanities For Quality of Care in Times of COVID - 19-Springer (2022)Sofronie MadalinNessuna valutazione finora
- POP June 10,2021 1Documento48 paginePOP June 10,2021 1Kerod AbebeNessuna valutazione finora
- Stress IncontinenceDocumento44 pagineStress IncontinenceswatisinghnigeriaNessuna valutazione finora
- PriapismDocumento14 paginePriapismNana Virtuoso EsselNessuna valutazione finora
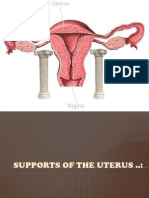
- Supports of The UterusDocumento20 pagineSupports of The UterusAshwin Prem Solomon100% (1)
- Pelvic Organ ProlapseDocumento9 paginePelvic Organ ProlapseSonny Dizon PareñasNessuna valutazione finora
- 50-Instrumental Vaginal DeliveryDocumento35 pagine50-Instrumental Vaginal Deliverydr_asalehNessuna valutazione finora
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDocumento8 pagineLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghNessuna valutazione finora
- Testicular TorsionDocumento20 pagineTesticular TorsionGAURAV100% (3)
- 04 Kelainan Bawaan Kasus Uroginekologi Dan Pengobatan SaatDocumento23 pagine04 Kelainan Bawaan Kasus Uroginekologi Dan Pengobatan SaatHerdinda Erudite Rizkinya100% (1)
- Cystoscopy: A Guide For WomenDocumento2 pagineCystoscopy: A Guide For Womenmonir61Nessuna valutazione finora
- 37 - Shock in ObstetricsDocumento22 pagine37 - Shock in Obstetricsdr_asaleh90% (10)
- Urinary IncontinenceDocumento112 pagineUrinary IncontinencePrabhakar KumarNessuna valutazione finora
- Pop QDocumento45 paginePop QObgyn Maret2016Nessuna valutazione finora
- Physiology of Micturition by DR - JawariaDocumento20 paginePhysiology of Micturition by DR - JawariaHifza Faqeer KambohNessuna valutazione finora
- Acute Urinary RetentionDocumento26 pagineAcute Urinary Retentionlukmankyubi100% (1)
- Neo BladderDocumento32 pagineNeo Bladderbelieveme030589Nessuna valutazione finora
- Bladder Substitution and Urinary DiversionDocumento58 pagineBladder Substitution and Urinary DiversionlifespotNessuna valutazione finora
- Obstetric Emergencies: DR - Himani Mehta MPT 2 Year Dept. of Gynae and Obstetrics CMC LudhianaDocumento26 pagineObstetric Emergencies: DR - Himani Mehta MPT 2 Year Dept. of Gynae and Obstetrics CMC LudhianarahulthedrNessuna valutazione finora
- Uterovesical FistulaDocumento42 pagineUterovesical Fistulakhadzx100% (2)
- Infections of Female Genital TractDocumento67 pagineInfections of Female Genital TractSana AftabNessuna valutazione finora
- Edited Maternal ProcedureDocumento45 pagineEdited Maternal ProcedureClare Alcober100% (1)
- Omphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Documento17 pagineOmphalocele Omphalocele: Perceptor: DR. AMRAN SINAGA, SP.B AUTHOR: Ida Ayu Ratna W, S.Ked (G1A214018)Rully Riyan DikaNessuna valutazione finora
- Suprapubic Catheter Bladder TrainingDocumento17 pagineSuprapubic Catheter Bladder TrainingOrmias PratamaNessuna valutazione finora
- Vovulusoriginal Copy 121028055752 Phpapp01Documento37 pagineVovulusoriginal Copy 121028055752 Phpapp01Bheru LalNessuna valutazione finora
- Surgical Problems in PregnancyDocumento37 pagineSurgical Problems in PregnancyCodillia CheongNessuna valutazione finora
- Genital FistulaeDocumento27 pagineGenital Fistulaeapi-3705046100% (1)
- Gynecological History Taking and ExaminationDocumento17 pagineGynecological History Taking and Examinationnmsiswaridewi100% (1)
- Hydrosalpinx MBDocumento30 pagineHydrosalpinx MBverhaniNessuna valutazione finora
- HMBDocumento41 pagineHMBakmal3501Nessuna valutazione finora
- Indication For Urethral CatheterizationDocumento2 pagineIndication For Urethral CatheterizationpawanNessuna valutazione finora
- Obstetric FistulaeDocumento24 pagineObstetric FistulaenyangaraNessuna valutazione finora
- Endoscopy and ColonosDocumento17 pagineEndoscopy and ColonosKim RamosNessuna valutazione finora
- Urinary Retention PostpartumDocumento5 pagineUrinary Retention PostpartumpaswordnyalupaNessuna valutazione finora
- Mechanism of MicturitionDocumento4 pagineMechanism of MicturitionGerardLum100% (2)
- Testicular TorsionDocumento20 pagineTesticular TorsionDarshan SinghNessuna valutazione finora
- CYSTOSTOMYDocumento60 pagineCYSTOSTOMYOepil KirickNessuna valutazione finora
- EPISPADIASDocumento16 pagineEPISPADIASAmina RajahNessuna valutazione finora
- KEMH Guidelines On Cardiac Disease in PregnancyDocumento7 pagineKEMH Guidelines On Cardiac Disease in PregnancyAyesha RazaNessuna valutazione finora
- Episiotomy & Episiorrhaphy: Dr. SumayyaDocumento35 pagineEpisiotomy & Episiorrhaphy: Dr. SumayyaMuhammad IbrahimNessuna valutazione finora
- Rupture of The Uterus: Associate Professor Iolanda Blidaru, MD, PHDDocumento21 pagineRupture of The Uterus: Associate Professor Iolanda Blidaru, MD, PHDOBGYN FKUI JAN-15Nessuna valutazione finora
- Total Pelvic ExenterationDocumento13 pagineTotal Pelvic ExenterationRirin Wahyuni100% (1)
- Carcinoma Gall BladderDocumento25 pagineCarcinoma Gall Bladderrajan kumarNessuna valutazione finora
- Genital FistulaeDocumento15 pagineGenital Fistulaesangeetha francisNessuna valutazione finora
- Xanthogranulomatous PyelonephritisDocumento14 pagineXanthogranulomatous PyelonephritisalaaNessuna valutazione finora
- EndometritisDocumento21 pagineEndometritisRoshni SunarNessuna valutazione finora
- Benign Disease of The UterusDocumento27 pagineBenign Disease of The UterusnyangaraNessuna valutazione finora
- Urinary System: Cytology, Histology, Cystoscopy, and RadiologyDa EverandUrinary System: Cytology, Histology, Cystoscopy, and RadiologyNessuna valutazione finora
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- TrunkDocumento86 pagineTrunkdr_asalehNessuna valutazione finora
- The Lower Limb: Pelvis, Thigh, Leg and FootDocumento27 pagineThe Lower Limb: Pelvis, Thigh, Leg and Footdr_asaleh100% (1)
- Elbow WristDocumento59 pagineElbow Wristdr_asalehNessuna valutazione finora
- Infertility IIDocumento58 pagineInfertility IIdr_asalehNessuna valutazione finora
- Head and NeckDocumento41 pagineHead and Neckdr_asalehNessuna valutazione finora
- Bones, Joints, MusclesDocumento37 pagineBones, Joints, Musclesdr_asalehNessuna valutazione finora
- Contents of PelvisDocumento38 pagineContents of Pelvisdr_asalehNessuna valutazione finora
- Disseminated Intravascular Coagulation in PregnancyDocumento8 pagineDisseminated Intravascular Coagulation in Pregnancydr_asaleh100% (1)
- 45-Fetal & Neonatal AsphyxiaDocumento35 pagine45-Fetal & Neonatal Asphyxiadr_asaleh100% (2)
- 51 EpisiotomyDocumento21 pagine51 Episiotomydr_asaleh100% (2)
- 36 - Acute Inversion of The UterusDocumento10 pagine36 - Acute Inversion of The Uterusdr_asaleh100% (1)
- 38 - HypofibrinogenaemiaDocumento8 pagine38 - Hypofibrinogenaemiadr_asalehNessuna valutazione finora
- 30 - Contracted Pelvis and Cephalopelvic DisproportionDocumento28 pagine30 - Contracted Pelvis and Cephalopelvic Disproportiondr_asaleh93% (14)
- 35 - Retained PlacentaDocumento11 pagine35 - Retained Placentadr_asalehNessuna valutazione finora
- Myocarditis With COVID-19 mRNA VaccinesDocumento34 pagineMyocarditis With COVID-19 mRNA VaccinesJorge Augusto Israel 狼Nessuna valutazione finora
- PainDocumento14 paginePainAmer Abdulla SachitNessuna valutazione finora
- HES 032 BSN - Lecture Comprehensive ExamDocumento47 pagineHES 032 BSN - Lecture Comprehensive ExamDIAZ, GIANNA D.Nessuna valutazione finora
- Acute Cholecystitis: From ER To Surgery: Riginal RticleDocumento5 pagineAcute Cholecystitis: From ER To Surgery: Riginal RticleKrystel Joy AuroNessuna valutazione finora
- CRITICAL THINKING EXERCISES Group 1 (1) 11Documento4 pagineCRITICAL THINKING EXERCISES Group 1 (1) 11Quinonez Anna MarieNessuna valutazione finora
- Tamoxifen PDFDocumento5 pagineTamoxifen PDFErza GenatrikaNessuna valutazione finora
- Cav Paliative Nursing CareDocumento17 pagineCav Paliative Nursing CareNamayanja SumayiyahNessuna valutazione finora
- Meeting 10 Guessing WordDocumento9 pagineMeeting 10 Guessing WordpramudyaNessuna valutazione finora
- King Abdulaziz University College of Pharmacy Clinical PharmacyDocumento3 pagineKing Abdulaziz University College of Pharmacy Clinical PharmacyHusnain AhmadNessuna valutazione finora
- Formulation, Optimizationand Evaluation of Sublingual Film of Enalapril Maleate Using 3 Full Factorial DesignDocumento9 pagineFormulation, Optimizationand Evaluation of Sublingual Film of Enalapril Maleate Using 3 Full Factorial DesignPRASANTA KUMAR MOHAPATRANessuna valutazione finora
- Avant Review Lesson 1-8 ECG Rhythm Strip InterpretationDocumento28 pagineAvant Review Lesson 1-8 ECG Rhythm Strip InterpretationphoebjaetanNessuna valutazione finora
- Save Standard Time To Alberta MLAs (2021 August 5)Documento9 pagineSave Standard Time To Alberta MLAs (2021 August 5)Save Standard TimeNessuna valutazione finora
- Qu Et Al. 2021Documento9 pagineQu Et Al. 2021Kassila SantosNessuna valutazione finora
- Essay About Health AwarenessDocumento2 pagineEssay About Health AwarenessYssah MalabananNessuna valutazione finora
- Drtbalu'S Otolaryngology Online: Acute LaryngitisDocumento3 pagineDrtbalu'S Otolaryngology Online: Acute LaryngitisAnish RajNessuna valutazione finora
- William McGuire (1981) Two-DimensionalDocumento14 pagineWilliam McGuire (1981) Two-DimensionalPAUL TIMMYNessuna valutazione finora
- Inhalation InjuryDocumento59 pagineInhalation InjuryElle LibalibNessuna valutazione finora
- ER تجميعة 3Documento27 pagineER تجميعة 3lclkNessuna valutazione finora
- American Society of Anesthesiologists Classification (ASA Class) - StatPearls - NCBI BookshelfDocumento3 pagineAmerican Society of Anesthesiologists Classification (ASA Class) - StatPearls - NCBI Bookshelfdaysesalg22599Nessuna valutazione finora
- Amodia - Purposive CommunicationDocumento7 pagineAmodia - Purposive CommunicationCLUVER AEDRIAN AMODIANessuna valutazione finora
- Definitions, Pathophysiology, and Evaluation of Chronic DiarrhoeaDocumento12 pagineDefinitions, Pathophysiology, and Evaluation of Chronic Diarrhoeamariana gamboa zapataNessuna valutazione finora
- Thyrooid GuidlineDocumento50 pagineThyrooid Guidlinepuskesmas tajurNessuna valutazione finora
- Bioplex 2200 System PanelsDocumento6 pagineBioplex 2200 System PanelsAbdulazizNessuna valutazione finora
- Stefania Boccia, Paolo Villari, Walter Ricciardi (Eds.) - A Systematic Review of Key Issues in Public Health (2015, Springer International Publishing)Documento294 pagineStefania Boccia, Paolo Villari, Walter Ricciardi (Eds.) - A Systematic Review of Key Issues in Public Health (2015, Springer International Publishing)Agus GunadiNessuna valutazione finora